What are ANAs?
Anti-nuclear antibodies (ANA) are a group of autoantibodies that are directed against self-antigens of the cell nuclei or cytoplasm.
What is the major principle of the ANA test?
In the indirect enzyme antibody technique, diluted patient samples are incubated with cells from the human epithelial type 2 cell line (HEp-2) that are fixed on a slide. These cells act as the substrate to allow specific binding of autoantibodies to cell nuclei. A stable antigen-antibody complex is formed if ANAs are present. Washing removes non-specific bound antibodies, and then the substrate is incubated with an anti-human antibody conjugated to horseradish peroxidase (HRP). A positive test results in the formation of a stable three-part complex consisting of an HRP-conjugated anti-human antibody bound to a human antinuclear antibody that is bound to a nuclear antigen. The slide is then incubated in the Colorzyme® color reagent, which contains an enzyme-specific substrate. The reaction between the enzyme labeled antibody, as described above, and the enzyme-specific substrate results in a color transformation visible on the slide using the typical bright-field microscope.
What type of cells are used in ANA testing?
The ANA test makes use of HEp-2 cells since these cells have large nuclei with high antigen expression.
Why is it important to utilize mitotic HEp-2 cells in ANA testing?
ANA testing makes use of mitotic HEp-2 cells since the cells improve sensitivity and make it easier to recognize or differentiate between patterns, especially if the evaluator is trying to distinguish between a speckled or homogeneous pattern. If the pattern is homogeneous, there will be solid staining of the chromosomes of the mitotic cells. If the pattern is truly speckled, the region outside of the chromosomes will show a fine speckled pattern. Mitotic cells also make it easier to distinguish between the peripheral pattern and nuclear membrane antibody. Mitotic cells should be visible on every field when viewed at 200x magnification or lower. Mitotic cells show a characteristic round cell shape with no detectable nuclear membrane. The chromosome region will generally show an irregular shape within the cell due to the lack of nuclear membrane and extreme constriction of the chromosomes. See circled mitotic cells below.
Example of metaphase
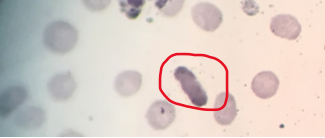)
Example of telophase
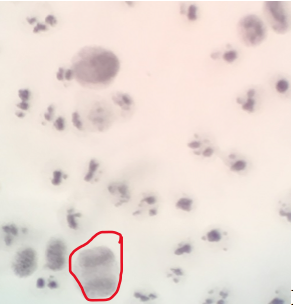)
Example of metaphase
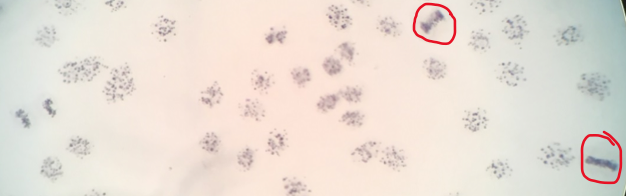)
What are the six phases of mitosis?
The six phases of mitosis are interphase, prophase, metaphase, anaphase, telophase, and cytokinesis.
Why are patient samples diluted and not run straight on the initial screening test?
Samples are diluted to avoid detecting low positive titers that are not clinically significant and can be seen in healthy individuals. A titer of ≥160 is usually considered clinically significant.
What quality control is used in the testing and how should the controls look when viewed on the microscope?
Positive, negative, and phosphate-buffered saline (PBS) controls are run on each slide. The homogeneous positive control should be used on the slides when performing the initial ANA screening. If a patient has been found to be positive on the screening and a titer needs to be performed, use the positive control provided by the manufacturer that is the same pattern as that of the patient. No matter the case, the positive control appears with dark blue-purple staining in the nuclei of the cells, with a clearly discernible pattern matching the pattern of the control used. The cytoplasm may or may not stain a light blue-purple color. Light blue-purple staining of both the cytoplasm and nucleus, but with no discernible pattern of nuclear staining, indicates a negative control. The PBS control is used to demonstrate non-specific staining and should not exhibit blue staining. If controls do not look as they should, the test is considered invalid and should be repeated.
When is a patient specimen considered positive?
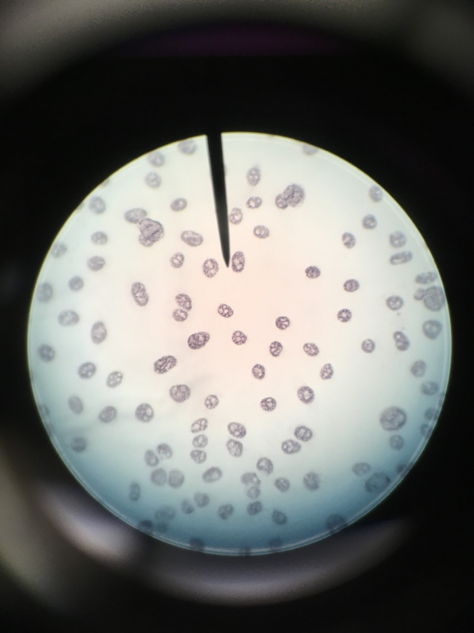
A patient specimen is considered positive if the nucleus shows a clearly discernible pattern of staining in the majority of the interphase cells.
When is a patient specimen considered negative?
A patient specimen is considered negative if nuclear staining is less than or equal to the negative control with no clearly discernible pattern. The cytoplasm may demonstrate weak staining with brighter staining of the nonchromosome region of mitotic cells but with no clearly discernible nuclear pattern.
If the initial screening test is found to be positive, how do you determine the titer?
The titer is determined by performing a doubling serial dilution using the initial 1:40 dilution and PBS as the diluent (e.g. 1:80, 1:160, 1:320, 1:640, 1:1280, 1:2560). Place the appropriate volume of each serial diluted sample onto a different well of a slide. Process the slide the same way as you would for the screening test. When reading the slide, begin reading with the well that contains the greatest dilution or most dilute sample and continue reading in descending order of dilutions to the smallest 1:40 dilution. The titer endpoint will be the first well in which a clearly discernible pattern is visible. The titer is reported as the reciprocal of the dilution. The pattern will also be reported. Low titers would be 40 or 80, medium titers would be 160 or 320, and high titers would be 640 or greater. The titer is used to determine the severity of the disease. The higher the titer, the more autoantibodies present.
What are the five most common ANA patterns?
The five most common ANA patterns are:
a. Speckled: A coarse or fine granular staining of the nucleus generally without staining of the nucleoli. The non-chromosome region of metaphase mitotic cells demonstrates staining, while the chromosome region is negative for stain.
b. Homogeneous: A solid staining of the nucleus with or without apparent masking of the nucleoli. The chromosome region of metaphase mitotic cells is clearly positive with a smooth or peripheral staining intensity greater than or equal to interphase nuclei.
c. Nucleolar: Large coarse speckled staining within the nucleus, generally less than 5 in number per cell with or without occasional fine speckles, 5-10 in number. The nonchromosome region of metaphase mitotic cells demonstrates strong staining, while the chromosome region may demonstrate faint staining. Anaphase and telophase cells may demonstrate similar staining to interphase nuclei.
d. Centromere: A discrete speckled staining pattern. The nuclear speckles are very discrete and usually some multiple of 46 (usually 23-26 speckles per nucleus). Because centromeres are constrictions where spindle fibers attach to chromosomes, mitotic cells will show the same speckling reaction in the chromosome region.
e. Peripheral: A solid staining, primarily around the outer region of the nucleus, with weaker staining toward the center of the nucleus. The chromosome region of metaphase mitotic cells is clearly positive with a smooth or peripheral staining intensity greater than or equal to interphase nuclei. The peripheral pattern is not investigated in this simulation.
Can a patient have a mixed pattern?
Yes, a patient can have a mixed pattern. This pattern can become more obvious when looking at a titrated sample.
Can a sample demonstrate nuclear and cytoplasmic staining with no distance nuclear pattern?
Yes, a sample can demonstrate nuclear and cytoplasmic staining with no distinct nuclear pattern. This is usually due to heterophile antibodies and should be reported as negative.
Does a positive ANA always indicate an autoimmune disease?
No, a positive ANA does not always indicate an autoimmune disease by itself. The physician must interpret results in conjunction with the patient's history, symptoms, physical findings, and other diagnostic tests.
What disease or condition is associated with each of the above patterns?
- Speckled: High titers are suggestive of systemic lupus erythematosus (SLE), mixed connective tissue disease, scleroderma, or Sjögren's syndrome-sicca complex; low titers may be suggestive of other connective tissue disease.
- Homogeneous or Peripheral: High titers are suggestive of SLE; lower titers are suggestive of SLE or other connective tissue diseases.
- Nucleolar: High titers are prevalent in scleroderma and Sjögren's syndrome.
- Centromere: Highly suggestive of the CREST (calcinosis, Raynaud phenomenon, esophageal dysmotility, sclerodactyly, and telangiectasia) syndrome variant of progressive systemic sclerosis (PSS).
Antinuclear antibodies are directed against different antigens. Given the following ANA patterns, what are those antigens?
- Speckled: Sm, RNP (ribonucleoprotein), Scl-70, SSA/Ro, SSB/La, and other antigen/antibody systems not yet characterized
- Homogeneous: dsDNA (double-stranded DNA) or nDNA (native DNA), DNP (deoxyribonuclear protein), histone
- Peripheral: dsDNA or nDNA, ssDNA (single-stranded DNA), histone
- Nucleolar: 4-6s RNAs and other nuclear antigens such as fibrillarin, RNA Polymerase I, NOR 90 (nucleolar organizer) and PM/Scl
- Centromere: Chromosomal centromere
Given the following data from the ANA colorzyme package insert, which pattern is most prevalent?
 Did you know that there is an indirect enzyme antibody technique for antinuclear antibody (ANA) testing that will allow you to view the slide using a bright-field microscope instead of a fluorescent microscope? So, what will you do in this simulation? You will perform the manual indirect enzyme antibody technique using the Immuno Concepts Colorzyme® ANA Test System. You will perform only the screening part of the procedure. You will not titer any positive ANAs in this simulation. This simulation will focus on four of the five basic ANA staining patterns.
Did you know that there is an indirect enzyme antibody technique for antinuclear antibody (ANA) testing that will allow you to view the slide using a bright-field microscope instead of a fluorescent microscope? So, what will you do in this simulation? You will perform the manual indirect enzyme antibody technique using the Immuno Concepts Colorzyme® ANA Test System. You will perform only the screening part of the procedure. You will not titer any positive ANAs in this simulation. This simulation will focus on four of the five basic ANA staining patterns.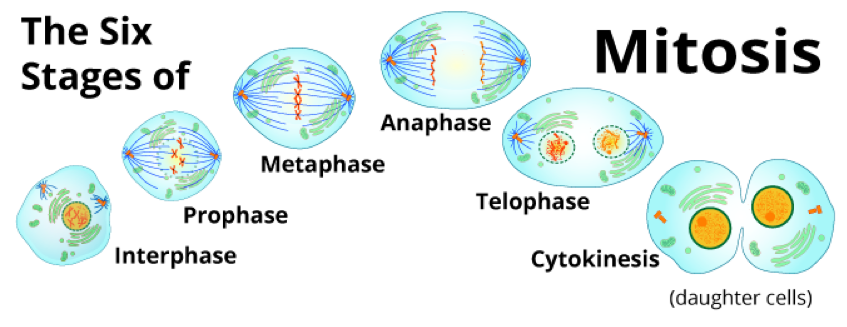)
) b. Homogeneous: A solid staining of the nucleus with or without apparent masking of the nucleoli. The chromosome region of metaphase mitotic cells is clearly positive with a smooth or peripheral staining intensity greater than or equal to interphase nuclei.
b. Homogeneous: A solid staining of the nucleus with or without apparent masking of the nucleoli. The chromosome region of metaphase mitotic cells is clearly positive with a smooth or peripheral staining intensity greater than or equal to interphase nuclei.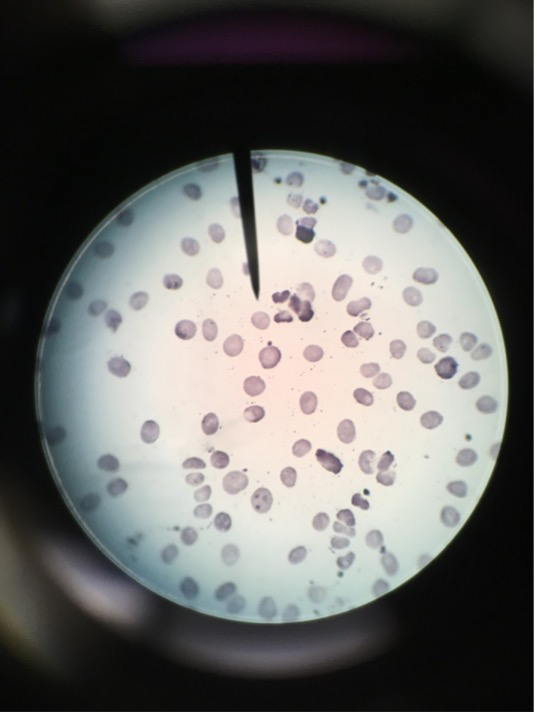) c. Nucleolar: Large coarse speckled staining within the nucleus, generally less than 5 in number per cell with or without occasional fine speckles, 5-10 in number. The nonchromosome region of metaphase mitotic cells demonstrates strong staining, while the chromosome region may demonstrate faint staining. Anaphase and telophase cells may demonstrate similar staining to interphase nuclei.
c. Nucleolar: Large coarse speckled staining within the nucleus, generally less than 5 in number per cell with or without occasional fine speckles, 5-10 in number. The nonchromosome region of metaphase mitotic cells demonstrates strong staining, while the chromosome region may demonstrate faint staining. Anaphase and telophase cells may demonstrate similar staining to interphase nuclei.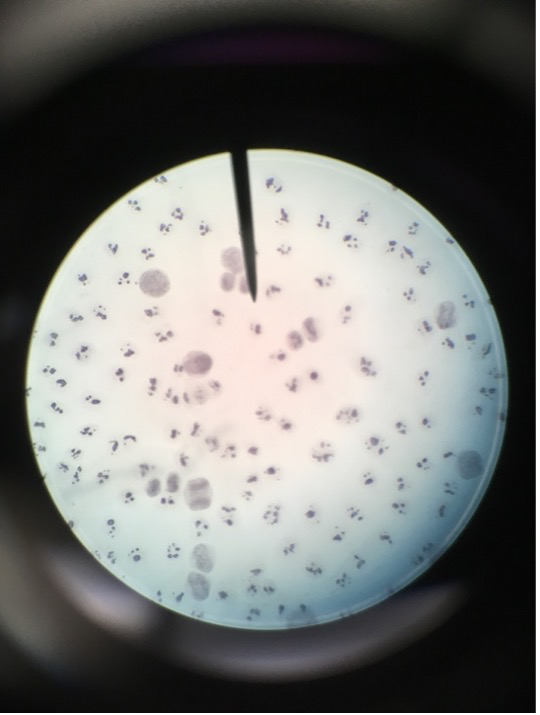) d. Centromere: A discrete speckled staining pattern. The nuclear speckles are very discrete and usually some multiple of 46 (usually 23-26 speckles per nucleus). Because centromeres are constrictions where spindle fibers attach to chromosomes, mitotic cells will show the same speckling reaction in the chromosome region.
d. Centromere: A discrete speckled staining pattern. The nuclear speckles are very discrete and usually some multiple of 46 (usually 23-26 speckles per nucleus). Because centromeres are constrictions where spindle fibers attach to chromosomes, mitotic cells will show the same speckling reaction in the chromosome region.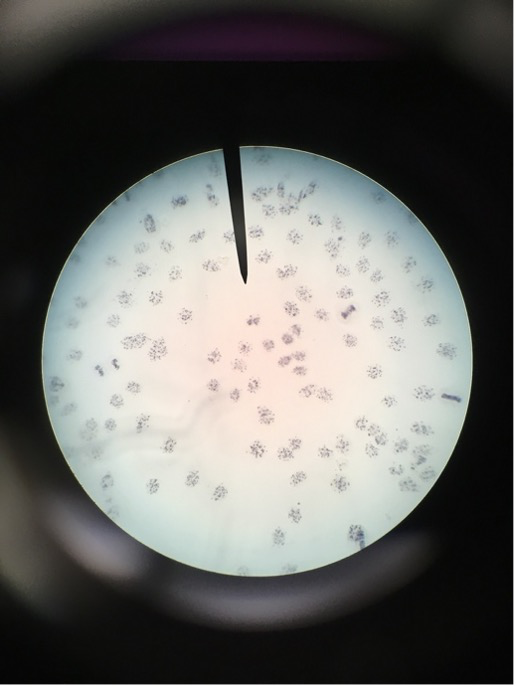) e. Peripheral: A solid staining, primarily around the outer region of the nucleus, with weaker staining toward the center of the nucleus. The chromosome region of metaphase mitotic cells is clearly positive with a smooth or peripheral staining intensity greater than or equal to interphase nuclei. The peripheral pattern is not investigated in this simulation.
e. Peripheral: A solid staining, primarily around the outer region of the nucleus, with weaker staining toward the center of the nucleus. The chromosome region of metaphase mitotic cells is clearly positive with a smooth or peripheral staining intensity greater than or equal to interphase nuclei. The peripheral pattern is not investigated in this simulation.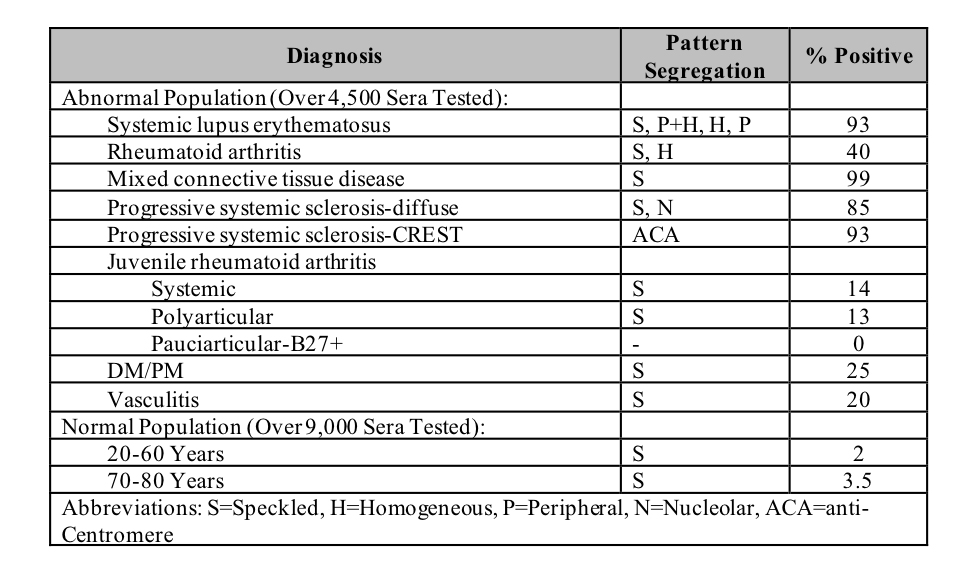)